
In the coming days, believers in all parts of the world are going to be faced with the question of whether or not to receive a vaccine against the novel SARS-CoV-2 virus, which is the source of the worldwide COVID-19 pandemic. A recent survey found that nearly 40 percent of respondents said they were unlikely to get such a vaccine even if it was approved.1
In the middle of a public health crisis, it might seem surprising that so many people are skeptical of the very solution that has been touted as the means of ending our nightmarish year of pandemic disruptions. Of course, there is nothing new under the sun; people have struggled with uncertainty about previous vaccines as well. As Christians we have an obligation to pursue all lawful means “to preserve our own life and the life of others.”2 It is legitimate when we assess any medical technology to ask if it will help preserve life. It is also critical that we “abhor what is evil; hold fast to what is good” (Rom. 12:9) and that we never “do evil that good may come” (Rom. 3:8).
Preservation of Life Concerns
As of this writing, it is estimated that the SARS-CoV-2 virus has infected around 71 million people, killing 1.6 million. In the United States the numbers are 16 million and 300,000 respectively.3 While far from the deadliest disease we have faced in history, COVID-19 is a serious health threat that is taxing our health-care capacity. It can be deadly especially among vulnerable populations like the elderly and those who have underlying health conditions. Even among younger people, consequences of the disease can linger well after the period of illness. So there is a legitimate health concern and the potential opportunity to preserve life if a vaccine is safe and effective.
One of the reasons there is so much skepticism about the safety of COVID vaccines is how rapidly they have been developed. The normal time frame for developing a vaccine is on the order of 10–15 years.4 The vaccines that are currently being tested have been developed in less than a year. This unprecedented timetable has rightly created concern in the minds of the public. After all, the federal program to produce these vaccines is named “Operation Warp Speed,” implying that we are discarding other considerations in order to prioritize speed.
A second reason for concern about these particular vaccines is that two of the leading candidates being tested (from Moderna and Pfizer) rely on a new technology that has no track record in previous vaccines. How can we know if these new technologies are safe, especially if we have sped up the timetable for approval?
To address these very real questions about safety, let us consider the technology being used as well as the testing process and the data we have so far. The Moderna and Pfizer vaccine candidates use a technology that has actually been in development since the 1990s as a way to deliver treatments to specific tissues.5 The basic concept, scientifically speaking, is to deliver messenger RNA (mRNA) packaged within small lipid droplets to particular cells in the body. The mRNA carries the genetic instructions to make a protein of interest in our cells. After the protein is made, the mRNA is degraded in the cells and the protein can “do its thing.”
When the genetic sequence of the new coronavirus was published in Jan. 2020, it was relatively simple for these companies to synthesize the mRNA to the major surface protein on the virus called the “Spike” or “S” protein. Since the mRNA delivery system was already functional, they were ready to begin preliminary experiments in animal systems very quickly.
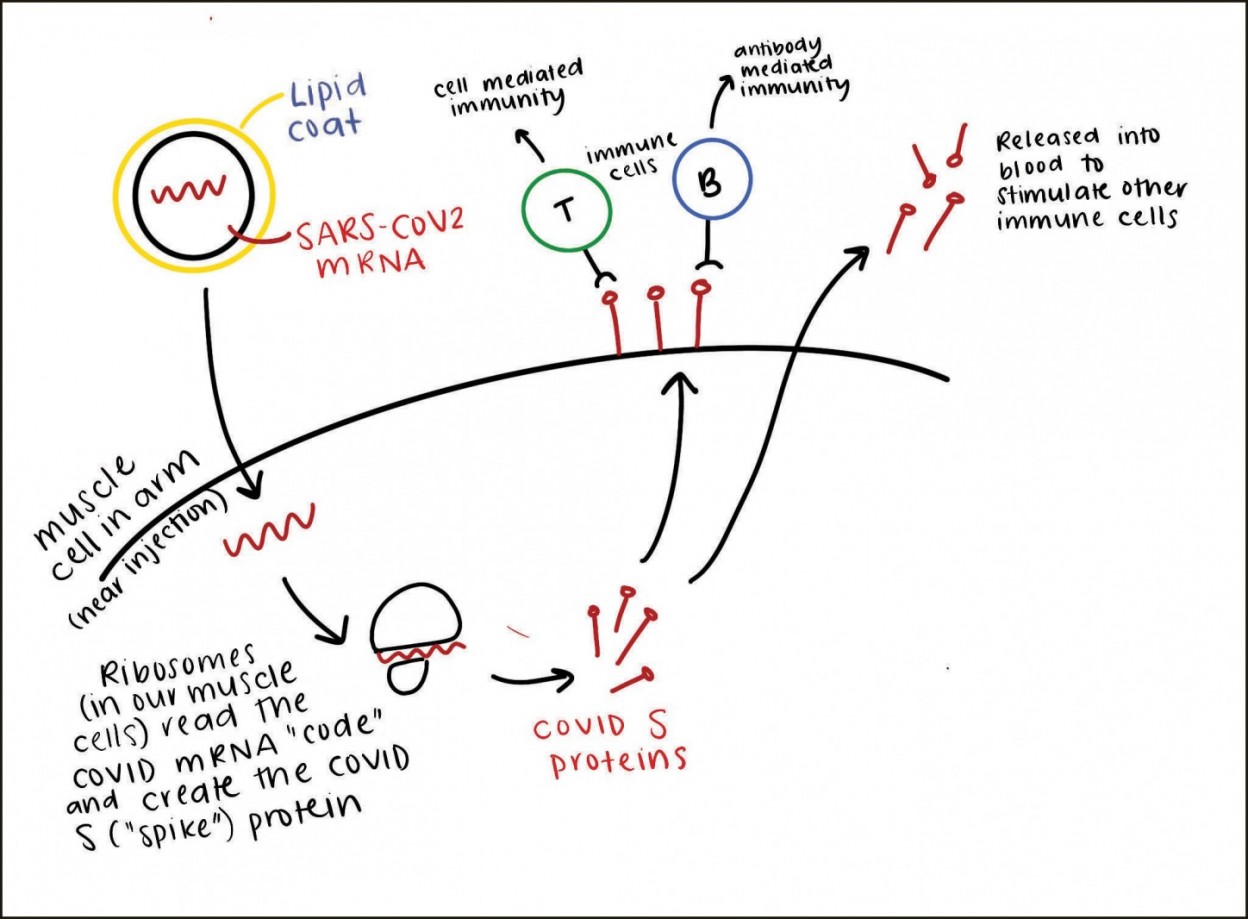
Conceptually, the mRNA technology seems safe. The mRNA, which codes for the S protein, is injected into the arm where it enters muscle cells (diagram). Those cells that take up the mRNA will make the viral S protein and put it on their surfaces, where it will be recognized by cells of the immune system. Those muscle cells will also release S protein into the bloodstream, where it further promotes an immune response. The relatively few “infected” muscle cells will themselves be killed, but not before triggering both arms of the immune system to recognize the virus. Since there is no actual virus being used (neither a killed virus, a weakened virus, nor a carrier virus), there is little risk to the recipient of the vaccine, and the immune response should be very specific to SARS-CoV-2.5
This explanation of the technology helps us see that it should be safe and effective. In addition, the nature of the technology itself explains why these vaccines could be developed so quickly.
The other important issue impacting the timetable is the investment of billions of dollars by the U.S. government. Normally, a company developing a vaccine does each phase of clinical trials sequentially, assesses outcomes, and then decides if it wants to risk more capital to proceed to the next step. Given that the process of getting approval for a treatment requires hundreds of millions of dollars, companies are cautious about moving to the next phase of testing.
Operation Warp Speed has removed the need to be cautious for these companies. By directly investing in the companies or by agreeing ahead of time to buy a certain number of units or to help with production, the government has paved the way for companies to test their vaccines with minimal financial risk. This has allowed the companies to combine Phase 1 and Phase 2 trials, which test safety in small numbers and then in larger numbers. As a result, companies have been able to move quickly to the all-important Phase 3 trials in which a vaccine’s safety and efficacy is tested in tens of thousands of patients.
The most important criteria for evaluating the life-preserving benefits of these vaccines is to look at the actual data from the Phase 3 trials, in which half of the participants are given the vaccine, half are given a placebo, and then all subjects are monitored. As of this writing both the Moderna candidate (30,000 adult subjects) and the Pfizer candidate (44,000 adult subjects) have reported a staggering 95% efficacy in preventing the disease with no significant side effects.7 As a result, these two candidates are headed for emergency-use authorization by the Food and Drug Administration by the middle of Dec. 2020. This designation allows a more rapid approval rate based on the importance of the medical emergency and the quality of the data. The Pfizer vaccine has already been approved in Great Britain, Bahrain, and Canada.
So, even though the process of development and testing in these vaccines has been greatly speeded up, the normal safety and efficacy tests have not been compromised. The data set for these vaccines is large and, at this point, fairly convincing. There are currently about a dozen different vaccines in Phase 3 trials with over 200 in other stages of development. It is impossible to evaluate the safety and efficacy of vaccines that have not been tested yet or that are being tested currently, but it is certainly reasonable and wise to do so when the data become available. It is worth noting here that the mRNA vaccines were tested in people 16 years and older, so they will not be approved for use in children until they are properly tested. Given the overall low lethality of the virus for most people, the decision to get the vaccine might be based more on loving one’s neighbor and seeking to preserve his life. The more people who are vaccinated and resistant to the virus, the more protection will be afforded the vulnerable in our society.
Moral Considerations
In recent years there has been greater opposition to the use of vaccines from various groups. Some Christians question vaccines for a number of reasons, some of which I’ve addressed briefly due to the limited scope and space of this article.
One misunderstanding some have is that vaccines “contain aborted baby parts.” This needs to be corrected. It is true that several vaccines commonly in use today (i.e., hepatitis A, chicken pox, rubella, rabies) as well as several of the COVID vaccines candidates in Phase 3 trials (i.e., AstraZeneca, Johnson & Johnson) use viruses that are grown in tissue culture cells that originally came from babies aborted several decades ago. These vaccines contain no fetal cells, but they may contain trace amounts of DNA from these cells.
We decry abortion as a sin against God and innocent human beings made in His image, but it is a stretch to say that using a vaccine that is grown in such cells makes us complicit in the evil of abortion. The creation of the four cell lines back in 1962, 1966, 1973, and 1985 was done for research purposes (not for vaccine development) after the abortions had already occurred. We cannot go back and undo the evil of the original abortions, but we need to be clear that the use of these cells in vaccine production today does not require or promote additional abortions. In the same way a person receiving a liver transplant from a donor who was murdered is not implicated in the murder, a person receiving a vaccine grown in these cells is not guilty of the abortion that made them available.
We do not minimize the moral qualms that some people, including fellow believers, have about the use of decades-old cell lines in vaccine production, but we also recognize that, as a general rule, we do not require believers to reject all technological advances that have any taint of sin in their development. If we did, we would have a very difficult time living in our world today. Virtually all of us use products like cars, computers, elevators, drinks, and medications that were created by companies founded by, funded by, or cooperating with the evil Nazi government in the 1900s, yet we do not consider our present-day use to be sin. Our responsibility is to avoid promoting evil or cooperating with evil in whatever decisions we make. In the case of life-saving vaccines, the use of cells derived as a secondary consequence of an evil act, is not itself evil.
Also, one of the benefits of having so many companies working on COVID vaccines is that there are alternatives that do not require fetal cell lines for their production. This is true for both the Moderna and the Pfizer mRNA vaccines, which should help those who have conscience concerns about fetal cells.
Some Recommendations
Vaccination is a tangible way to preserve our own life and the life of others. But that does not mean that every vaccine is equally safe or effective. There have been rare instances throughout history when vaccines have caused serious complications. These situations were identified and remedied, which should give us confidence that there is a functional system in place to catch any significant side effects. It is altogether wise to evaluate the data as it comes in for the new COVID vaccines—especially in light of the expedited timetable.
At this point, preliminary data look very promising for the two mRNA candidates, so that is encouraging. We currently have data on tens of thousands of people taken over several months. As these vaccines are given more widely, we will eventually have data on millions of people, which will allow us to see if there are less common side effects that would not be caught with the smaller sample size. In addition, we will get safety and efficacy data over longer periods of time. Although these vaccines are being developed and tested rapidly, it does not appear that there are any sacrifices being made in terms of ascertaining their quality. These facts suggest that we can honor God by receiving a COVID vaccine, which will promote our own health and that of our neighbor.
Since this article is a snapshot being taken during a rapidly moving situation, you ought to find reliable sources of information that will allow you to evaluate new data as it becomes available. In all things, let us pray for the wisdom of Christ who is the power and wisdom of God (1 Cor. 1:24).
Resources for further study
Children’s Hospital of Philadelphia’s Vaccine Education Center
Charlotte Lozier Institute: Science and Statistics for Life
“Amid COVID-19, Pro-Lifers Push to Avoid Abortive Fetal Cells in Medicine” by Rebecca Randal at Christianity Today
“Vaccines and Doubly Remote Cooperation in Evil” by Matthew Schneider at Public Discourse
Dr. Jay Wile on RNA vaccines for COVID
Rich Holdeman is a pastor at the Bloomington, Ind., RPC. He is also senior lecturer in the department of biology at Indiana University where he teaches classes in cell biology, genetics, and disease biology.
-
Pew Research Center, Dec. 2, 2020. ↩︎
-
Westminster Shorter Catechism Question 68 on what keeping the sixth commandment requires. ↩︎
-
According to Worldometer accessed on Dec. 11, 2020. ↩︎
-
The History of Vaccines website accessed on Dec. 8, 2020. ↩︎
-
“RNA Vaccines: Harnessing God’s design to help prevent sickness, but will the new vaccine technology alter our DNA?”, Creation Ministries International, accessed Dec. 11, 2020. ↩︎